

- Blog
- 10 Apr 2026

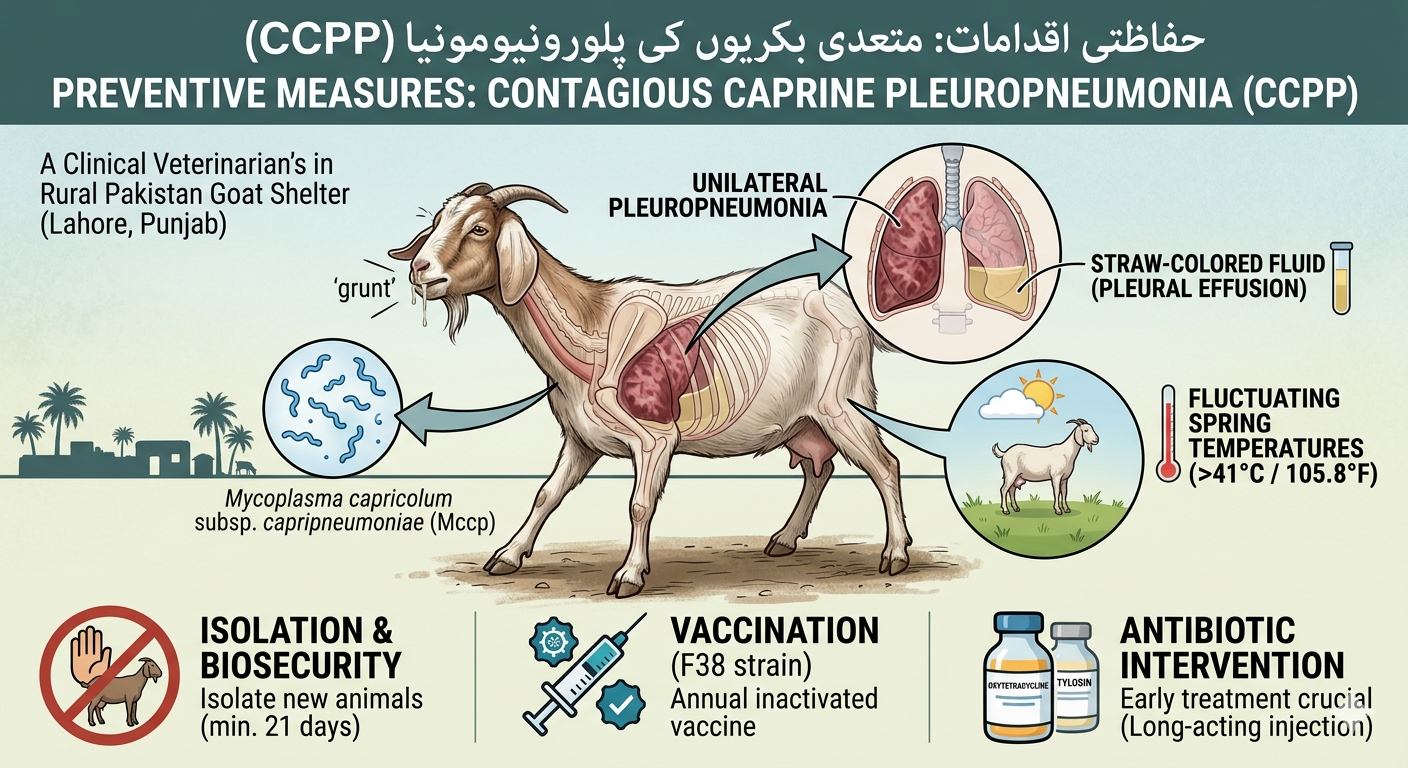
Because of the high morbidity (up to 100%) and mortality (up to 80-100%) rates associated with Contagious Caprine Pleuropneumonia (CCPP), it remains one of the most economically devastating respiratory diseases for goat populations globally.
Caused by the bacterium Mycoplasma capricolum subsp. capripneumoniae (Mccp), it is strictly a disease of goats and does not cross over to sheep or cattle, though it is highly infectious within a herd.
Clinical Signs to Monitor
The disease typically follows an acute or peracute course. In clinical settings, you will often observe:
-
High Fever: Temperatures often reaching $41\text{°C}$ ($105.8\text{°F}$) or higher.
-
Respiratory Distress: Labored breathing, painful coughing, and a distinctive "grunting" sound on expiration.
-
Characteristic Posture: Goats may stand with their forelegs wide apart and neck extended to facilitate breathing.
-
Nasal Discharge: Initially serous, becoming mucopurulent as the disease progresses.
Pathological Hallmarks (Post-Mortem)
If a necropsy is performed, the findings are usually confined to the thoracic cavity:
-
Unilateral Pleuropneumonia: Interestingly, the hepatization (consolidation) of the lung tissue is frequently restricted to just one lung.
-
Straw-Colored Fluid: Accumulation of excessive pleural fluid (up to $500\text{ ml}$) that often coagulates into gelatinous masses.
-
"Marbling" Effect: While less pronounced than in cattle with CBPP, the thickened interlobular septa can give the lungs a marbled appearance.
Management & Control Strategies
-
Strict Biosecurity: CCPP is primarily spread through aerosol droplets. Isolation of new animals for at least 21 days is the gold standard for prevention.
-
Vaccination: In endemic areas, an inactivated vaccine (often using the F38 strain) is highly effective. Immunity generally lasts about a year.
-
Antibiotic Intervention: Early treatment is vital. Research and clinical data show that Tetracyclines (specifically long-acting Oxytetracycline) and Macrolides (like Tilmicosin or Tylosin) are effective if administered before extensive lung consolidation occurs.
-
Movement Control: Because the disease is often introduced by subclinical carriers, restricting the movement of animals from known infected zones is the most effective way to prevent regional spread.
Clinical Tip for Spring
With the fluctuating temperatures typical of April, environmental stress can exacerbate subclinical infections. Ensuring goats have access to dry, well-ventilated housing without drafts can significantly reduce the severity of a sudden outbreak.
Building on the clinical basics, here are the more technical details regarding the epidemiology, advanced diagnostics, and specific treatment protocols for Contagious Caprine Pleuropneumonia (CCPP).
1. Advanced Diagnostics (The "Gold Standard" vs. Field Reality)
Diagnosing CCPP is notoriously difficult because M. capricolum subsp. capripneumoniae (Mccp) is extremely fastidious and slow-growing, often taking over 15 days to culture.
-
Preferred Sample: Pleural fluid or lung tissue from the interface of healthy and hepatized areas.
-
PCR Testing: This is the current preferred method due to speed and specificity. It can differentiate Mccp from other "Mycoides cluster" pathogens like M. mycoides subsp. capri (Mmc), which can cause similar-looking symptoms.
-
Latex Agglutination Test (LAT): A highly valuable pen-side test. It can detect antibodies in the field within minutes, making it ideal for rapid screening during an outbreak.
-
Competitive ELISA (c-ELISA): Typically used for international trade and large-scale surveillance to confirm a "disease-free" status.
2. Differential Diagnosis
CCPP is frequently confused with other major respiratory killers. Key differentiators include:
-
PPR (Peste des Petits Ruminants): Unlike CCPP, PPR often presents with diarrhea and ocular/nasal crusting.
-
Pasteurellosis: Usually causes bilateral pneumonia, whereas CCPP is classically unilateral.
-
MAKePS Syndrome: Caused by Mmc, this presents with Mastitis, Arthritis, Keratoconjunctivitis, Peritonitis, and Septicemia—lesions that are absent in true CCPP.
3. Updated Therapeutic Protocols (2026 Trends)
While older protocols relied solely on Oxytetracycline, recent clinical evaluations (especially in high-value goats) suggest a combination therapy approach for better recovery rates:
|
Medication Type |
Recommended Drug |
Dosage/Notes |
|---|---|---|
|
Primary Antibiotic |
Tylosin |
Often shows faster clinical recovery and lower relapse rates than tetracyclines. |
|
Secondary Option |
Enrofloxacin |
A potent alternative, especially in cases where resistance to tetracyclines is suspected. |
|
Anti-Inflammatory |
Meloxicam |
Crucial for reducing pleurodynia (chest pain) and lowering fever (0.5 mg/kg). |
|
Anti-Allergic |
Pheniramine Maleate |
Used in combination to manage the inflammatory cascade in the lungs (1.0 mg/kg). |
Export to Sheets
4. Economic & Epidemiological Impact
-
The "Silent Carrier" Problem: Animals that survive the acute phase can become subclinical carriers. They may show no symptoms but will shed the bacteria during periods of stress (like the fluctuating spring weather mentioned earlier), triggering new outbreaks.
-
Yield Loss: Beyond mortality, CCPP causes a permanent reduction in production. For fiber-producing breeds (like Pashmina goats), a 30% reduction in yield is common in survivors.
+1
-
Wild Ruminant Reservoir: Recent data has confirmed Mccp in wild species such as the Nubian Ibex and Gazelles, which can complicate eradication efforts in regions where domestic goats share grazing lands with wildlife.
5. Vaccination Nuance
The F38 strain inactivated vaccine is the standard. However, it is important to note that vaccination is prophylactic. If a goat is already in the incubation phase, the vaccine will not prevent the disease. Annual revaccination is mandatory in endemic zones to maintain herd immunity.
